What Is Prediabetes? A Plain-English Explanation Of HbA1c, Fasting Glucose, And Insulin Resistance
What Is Prediabetes? A Plain-English Explanation Of HbA1c, Fasting Glucose, And Insulin Resistance
You went for a routine check-up. Your doctor said something like “your sugar is a bit high — you have prediabetes.” Maybe they suggested losing weight, or scheduled another test in six months. You left without a clear picture of what is actually going on inside your body, what the numbers mean, or what to do this week.
This article gives you that picture in plain language. No alarm, no minimization. Just the mechanism, the numbers, and the levers you can pull.
The one-sentence definition
Prediabetes means your blood sugar is consistently higher than the healthy range, but not yet high enough to be called type 2 diabetes. It is a warning state, and in most people it is reversible.
The three numbers your doctor uses
There are three different blood tests that can put you in the prediabetes range. You only need one to qualify, but doctors often run two of them together for a clearer picture.
HbA1c — the three-month average. HbA1c (sometimes written A1c or “glycated hemoglobin”) measures how much sugar has been stuck to your red blood cells over the past 8–12 weeks. Because red blood cells live about three months, this single number reflects the average of all your blood sugar readings during that time.
- Normal: below 5.7%
- Prediabetes: 5.7%–6.4%
- Type 2 diabetes: 6.5% or higher
A single morning meal cannot move HbA1c. A pattern of meals over months can.
Fasting plasma glucose (FPG) — your morning baseline. This is your blood sugar after at least 8 hours without food, usually drawn first thing in the morning before breakfast. It tells you how well your body manages glucose at rest, when no food is competing for attention.
- Normal: below 100 mg/dL (5.6 mmol/L)
- Prediabetes: 100–125 mg/dL (5.6–6.9 mmol/L)
- Type 2 diabetes: 126 mg/dL (7.0 mmol/L) or higher
A fasting glucose of 105 is not a typo or a one-off. If repeated, it is the body saying: even after a full night of no food, my pancreas and liver are not putting glucose where it belongs.
Oral glucose tolerance test (OGTT) — the stress test. You drink a measured sugary solution (75 g glucose), then have your blood sugar checked two hours later.
- Normal: below 140 mg/dL (7.8 mmol/L) at 2h
- Prediabetes: 140–199 mg/dL (7.8–11.0 mmol/L) at 2h
- Type 2 diabetes: 200 mg/dL (11.1 mmol/L) or higher at 2h
OGTT catches “hidden” prediabetes — people whose fasting numbers look fine but whose body cannot handle a sugar load efficiently. It is the most sensitive test, but also the most cumbersome, so it is used less often in routine care.
If your number sits in any one of these prediabetes ranges on two separate occasions, the diagnosis applies.
What is actually happening inside the body
The numbers are the symptom. The mechanism is insulin resistance.
Here is the simple version. When you eat carbohydrates, your blood sugar rises. Your pancreas releases insulin, a hormone that tells your muscles, liver and fat cells to absorb that sugar so it does not stay in the bloodstream. In a healthy person, this happens cleanly: sugar in, insulin out, sugar absorbed, blood glucose returns to baseline within two hours.
In someone with insulin resistance, the cells stop responding well to insulin’s signal. The pancreas notices and pumps out more insulin to push the message harder. For a while this works — your blood sugar still comes back to baseline — but it requires more and more insulin to do the same job. This is the silent phase. You probably feel tired in the afternoon, gain weight around the middle more easily, and have stubborn cravings, but your fasting glucose still looks normal.
Eventually the pancreas cannot keep up. Glucose lingers in the blood longer. Fasting numbers drift up. HbA1c creeps from 5.4 to 5.7 to 5.9. That is the moment you get the prediabetes label.
So prediabetes is not a small amount of diabetes. It is a late symptom of years of insulin resistance.
Why this matters more than the label
Two things follow from understanding the mechanism.
First, prediabetes does not “turn into” diabetes randomly. It progresses if insulin resistance keeps getting worse. Without intervention, roughly 5–10% of people with prediabetes develop type 2 diabetes each year. Within 5–10 years, more than half progress.
Second, and more usefully — prediabetes is reversible. The same lever that pushed it up (insulin resistance) can be pushed back down. Multiple large randomized trials, including the U.S. Diabetes Prevention Program, have shown that lifestyle changes reduce progression to type 2 diabetes by 58% over three years. That is a larger effect than metformin produces in the same trials.
The practical levers
You will see lots of generic “eat better, exercise more” advice. Here is what actually moves the underlying mechanism, in rough order of impact per hour invested.
Lever 1: lower the glycemic load of your meals, not just calories. Insulin resistance is provoked most by foods that spike blood sugar quickly. The metric here is glycemic load (GL), which combines how fast a food raises blood sugar (glycemic index) with how much carbohydrate it contains. A meal with GL under 12 per portion keeps the spike — and the insulin response — modest. White rice, sweet drinks, mainstream breakfast cereals, and most “quick” snacks are very high-GL. Lentils, oats, plain yogurt, eggs, vegetables, most berries, and intact whole grains are low-GL. (For a deeper breakdown of GL vs GI, see glycemic load vs glycemic index.)
Lever 2: move within 30 minutes of eating. A 15-minute walk after a meal lowers the post-meal glucose peak by 15–30% in most studies. Muscle pulls glucose out of the blood without needing insulin when it is contracting. This is the cheapest single intervention available to a person with prediabetes — no equipment, no skill, no cost.
Lever 3: eat protein at every meal, especially breakfast. A breakfast with 25–30 g of protein blunts the morning insulin spike, reduces lunchtime cravings, and improves muscle insulin sensitivity over weeks. Eggs, plain Greek yogurt, cottage cheese, leftover meat or fish, tofu, or a protein shake all qualify. A pastry-and-coffee breakfast is the worst possible start to a day for someone with prediabetes.
Lever 4: sleep 7+ hours, consistently. One night of poor sleep measurably reduces insulin sensitivity the next day. Chronic short sleep (under 6 hours) raises HbA1c independently of diet. If your sleep is broken, fix it before optimizing your diet — the diet effort works better when you are rested.
Lever 5: lose 5–7% of body weight. This is the threshold that produces measurable HbA1c drops in trials. You do not need to reach a “normal” BMI. Going from 92 kg to 86 kg is enough to drop most people out of the prediabetes range, if the weight loss is sustained.
Lever 6: build muscle. Larger, more active muscles soak up more glucose and act as a sink for blood sugar. Two strength sessions per week, focused on big movements (squats, rows, push-ups, deadlifts), is the minimum useful dose. This is a slower-acting lever — effects show up after 8–12 weeks — but it raises the ceiling on every other intervention.
You do not need all six at once. Picking one and doing it for two weeks is more effective than trying to overhaul everything.
What to ignore
Three things commonly distract people just diagnosed with prediabetes.
“Just cut sugar.” Cutting added sugar helps, but white bread, white rice, instant oats and most fruit juices spike blood sugar just as hard. The rule is total fast carbohydrate per meal, not just teaspoons of table sugar.
“Eat tiny meals every 2 hours.” This was 1990s advice. For a person with insulin resistance, every meal is an insulin event. Three meals with no snacking — what is sometimes called time-restricted eating — usually produces lower fasting glucose than six small meals.
“Wait six months and re-test.” If your test came back in the prediabetes range, that is the moment to start, not the moment to wait. Six months of no change usually means six months of slow drift upward.
How to track whether you are moving the needle
You do not need a continuous glucose monitor (though they are useful if you can afford one). Three cheap signals tell you whether your interventions are working.
- Re-test HbA1c at three months. That is one full red-blood-cell cycle. A drop of even 0.2% (e.g., 6.0 to 5.8) is meaningful — it means the trend reversed.
- Track your morning fasting glucose with a finger-stick meter once a week. Do it at the same time, same conditions. A two-month downward trend is the signal you want.
- Track post-meal energy. When insulin sensitivity improves, the afternoon crash starts disappearing. That subjective signal often shows up before the lab numbers move.
If you want a structured way to do all this without keeping a paper journal, the Logi app shows the glycemic load of each meal you photograph, predicts your blood sugar curve for the next three hours, suggests lower-GL swaps, and tracks the trends across weeks. It is built for exactly this — the prediabetes window when small changes still produce big results.
A realistic timeline
If you act on the levers above with reasonable consistency, here is roughly what to expect.
- Weeks 1–2: post-meal energy stabilizes. Cravings diminish. You sleep slightly better.
- Weeks 3–6: clothes fit a little looser, especially around the middle. Weight may not have moved much yet — visceral fat goes first and weighs less than subcutaneous fat.
- Months 2–3: fasting glucose drops 5–15 mg/dL on average. HbA1c at the three-month re-test is typically 0.2–0.5% lower.
- Months 4–6: if you are in the upper prediabetes range, you may move back into normal. If you started higher (e.g., HbA1c 6.3%), you are likely still in prediabetes range but trending down.
This is not fast. But it is real, repeatable, and has been replicated in dozens of clinical trials. The alternative — doing nothing — has a much more predictable trajectory in the wrong direction.
What to do this week
Pick one lever. Just one.
- Walk 15 minutes after dinner every day.
- Or replace your breakfast with 30 g of protein for seven days.
- Or do a morning fasting glucose test on Monday and again on Sunday, to see the natural variation.
Two weeks of one change beats two days of trying to do everything. Prediabetes is a slow problem. The fix is also slow. But you are in the window where slow still works.
Related reading
- Insulin Resistance Diet: What to Eat and What to Avoid in 2026
- Glycemic Load vs Glycemic Index: Why GL Matters More for Insulin Resistance
- Why You’re Not Losing Weight Even When You Eat Less
- Signs of Insulin Resistance: A 12-Question Self-Check
This article is educational and is not a substitute for medical advice. If you have been diagnosed with prediabetes, work with your doctor on a plan that fits your full medical picture.
Take control of your blood sugar
Scan your meals, track glycemic load, and see your patterns — all in one app.
開始免費試用 →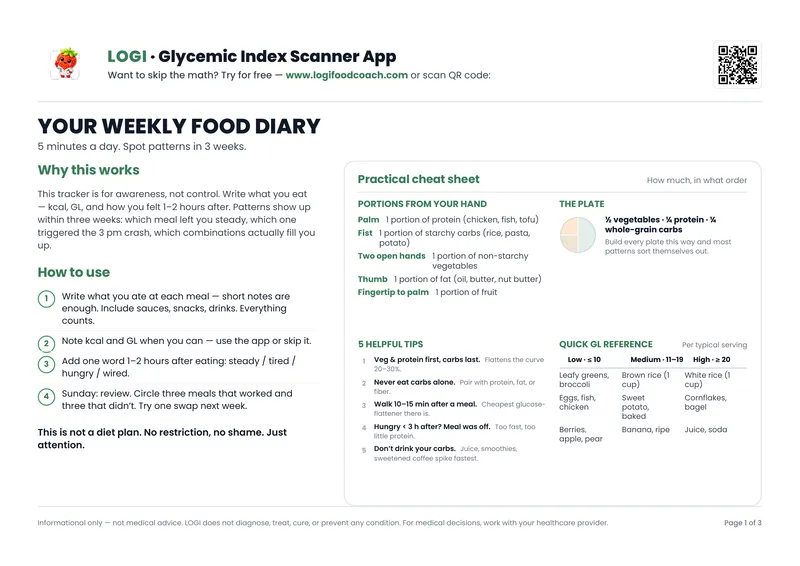
免費PDF — 3頁
每週飲食日誌
記錄飲食、升糖負荷與心情。3週內發現規律。
無垃圾郵件。隨時取消訂閱。